Britney Bell and Jue Wang
Received: November 09, 2019; Published: December 06, 2019
Abstract
Background: Tumor lysis syndrome is a common oncologic emergency which has been well documented in patients suffering from hematologic malignancies. However, it is rarely reported in patients with solid tumors, even more rarely in patients with breast cancer. Many emergency room physicians, internists, even oncologists are not aware that TLS can actually occur in breast cancer. The objective of this study was to investigate the clinical characteristics and outcomes of TLS, a rare but life-threatening complication in breast cancer.
Methods: Retrospective literature review and pooled analysis.
Results: Twenty cases of TLS were identified in patients with breast cancer (19 case in published literature and 1 additional case from our tumor registry). The median age of patients was 57 years (31 – 94) with a female to male ratio of 19:1. All patients had extensive metastatic disease at the time of presentation, with visceral metastases documented in 100% of TLS cases. The in hospital mortality rate of entire cohort was 68%. The mortality rate for the patients developing treatment related TLS and spontaneous TLS were 50% and 75% respectively.
Conclusion: TLS in breast cancer can occur both after treatment and spontaneously and is associated with very high mortality.
Our findings underscore the importance of heightened awareness, risk assessment and early prevention of this previously underrecognized oncologic emergency
Keywords: Breast Cancer; Tumor Lysis Syndrome (TLS); Oncologic Emergency; Mortality
Introduction
Tumor lysis syndrome (TLS) is the most common oncological emergency that results in severe metabolic abnormalities, including hyperkalemia, hyperphosphatemia, hyperuricemia and hypocalcemia, in patients with rapidly proliferating and chemosensitive malignancies, such as acute lymphoblastic leukemia or high-grade lymphoma [1,2]. These metabolic abnormalities are responsible for an array of sequelae, the most common which are cardiac arrhythmias, acute renal failure, seizures, and sudden death. Although TLS is a well recognized clinical problem in hematological malignancies, it continues to remain understudied in solid tumors and until recently [2-17].
Between 2017 and 2019, we treated three cases of TLS associated with breast cancer. We consider these clinical observations deserved further investigation.
Objective of the Study
The objective of this study was to examine the available published information on clinical characteristics, management and outcomes of TLS in patients with breast cancer.
Patients and Methods
Literature search strategy
Systematic review of the literature was performed by first searching PubMed for “tumor lysis syndrome” and “breast cancer”. The identified case reports and abstracts were reviewed and additional articles of interest were identified from reference lists.
Data collection and statistical analysis Information regarding the patient (age at diagnosis, presentation, and comorbidities), the tumor (histology, grade and AJCC stage), radiologic investigations, treatment modalities (surgery, radiation and systemic therapy), and the outcome (response, adverse events, vital status) were recorded, when available. Descriptive statistics, such as frequency counts, medians, and ranges, were used to characterize the pooled sample.
Results
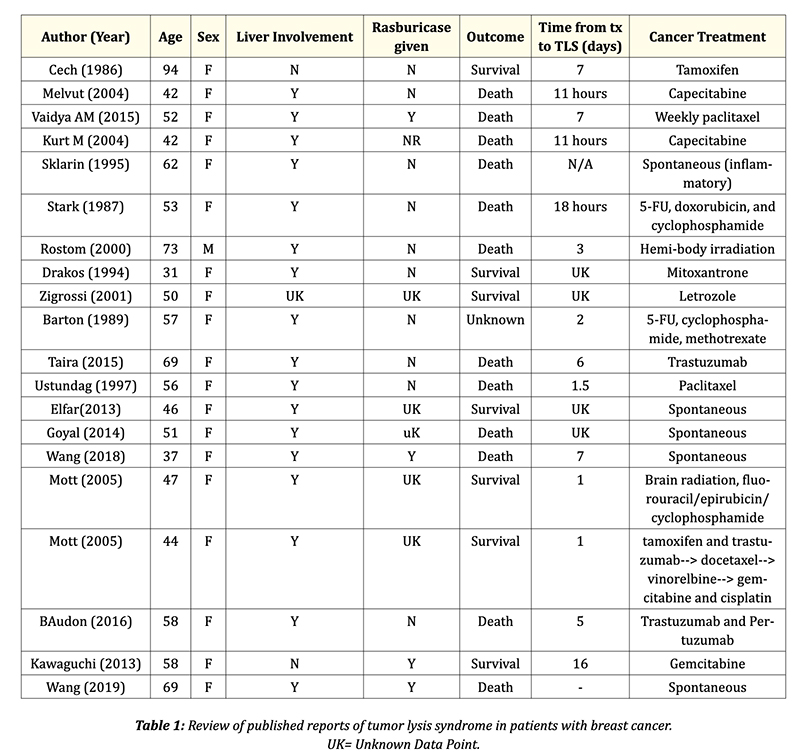
Eighteen published case reports associated with metastatic breast cancer with total 19 cases of TLS (16 cases of treatment related and 3 cases of spontaneous TLS) were identified. In addition, we identified one case of spontaneous TLS in our institutional database. The final cohort consistent of a total 20 breast cancer patients with TLS.
The demographic feature, clinicopathologic features, symptoms and survival outcomes of 20 cases of TLS in breast cancer were summarized in table 1. The mean age of patients was 57 years (31 – 94) with majority patents were female (95%). All cases were adenocarcinoma (one with inflammatory breast cancer). In all cases, patients presented with metastatic disease with all patients having visceral metastases and 17 (85%) of the patients having liver metastases. Four patients (20%) in the pool of case reports developed spontaneous TLS, while sixteen of the patients (80%) developed TLS after receiving some type of active cancer treatment. Among them, eight of the patients (50%) developing treatment related TLS received chemotherapy alone which included capecitabine, paclitaxel, 5-FU, doxorubicin, methotrexate, gemcitabine and cyclophosphamide. Two of the patients (12.5%) that developed TLS post treatment received hormone therapy (tamoxifen and letrozole) prior to admission. Monoclonal antibodies, specifically trastuzumab and pertuzumab, was responsible
for two out of the sixteen cases of treatment related TLS. One patient developed TLS after receiving a sequence of hormone therapy, immunotherapy, and chemotherapy. Hemi-body irradiation was responsible for one case of treatment related TLS, while there was also one case of chemotherapy and radiation, leading to the development of TLS. All cases were treated with aggressive supportive measures, and three patients received rasburicase.
The mortality rate was 50% among sixteen cases of treatment related TLS, with a median survival from diagnosis of TLS to death was 2 days (range 0.5-16). The mortality rate was 75% in the four patients with spontaneous TLS.
Discussion
Though well-documented in hematological malignancies, TLS was considered relatively rare in other solid tumors [3-5]. Our current study show TLS in breast cancer does indeed occur and is a real, under-recognized oncologic emergency. Although the true incidence of TLS in breast cancer is difficult to assess. It is important to identify reasons for this under recognition to further equip physicians in pro viding optimal care to patients. One of these reasons, is the fact that many emergency room physicians, internists, even oncologists are not aware TLS can actually occur in breast cancer, therefore, TLS is not included in their initial differential diagnosis, specifically in patients presenting with acute renal failure. Between 2017 and 2019, our group treated three cases of spontaneous TLS associated with metastatic breast cancer. In both cases, the diagnoses were delayed due to failure to consider TLS as potential diagnosis at emergency room. We postulated TLS in breast cancer may be under diagnosed and under-reported. Hopefully the finding from our analysis can convince those skeptical whether TLS is a true phenomenon.
Several findings from this study are noteworthy. First, TLS generally occurs in patients with advanced stage breast cancer with large disease burdens. Distant metastases were documented in all TLS cases in this study, more specifically 90% of cases reported liver metastasis. Secondly, TLS in breast cancer, particularly spontaneous TLS, carries a worse prognosis when compared to hematologic malignancies [18-25,26]. The lacks of awareness of risk of TLS in breast cancer in the new era of targeted therapy, delay in diagnosis and suboptimal management likely contribute to the observed high mortality. Urgent education efforts should be made to increase the awareness for this rare but potentially life-threatening oncologic emergency. Another interesting observation is one patient had inflammatory breast cancer with known aggressive biological behaviors and rapid proliferation rate. The current guidelines and consensus on diagnosis and management of TLS were based on previous experience on hematologic malignancies and established at a time when effective therapies for solid
tumors were not available, refine the risk stratification and management TLS strategy in the new targeted therapy and immunotherapy era is necessary based on recent findings [2-5]. For patients with high burden of metastatic disease especially elderly cancer patients with extensive liver metastases, it is critical to monitor patients’ electrolytes and renal function at least weekly during the first cycle of systemic therapy.
Limitation of the Study
Our study has several limitations. Due to the inherent nature of retrospective studies, we were not able to fully assess factors such as individual patient’s performance status, and comorbid conditions that may impact the outcome of TLS. A larger sample size would also provide further insight into the stratification of risk of patients based on therapy type prior to TLS development and presence of rasburicase as an aggressive treatment option. Despite the limitations, the present study provides the most updated real world insight regarding the diagnosis and outcomes of TLS in patients with metastatic breast cancer. Our study will contribute to the evolving understanding of TLS in solid tumors and have implications for future cancer treatment paradigms in target therapy era.
Conclusion
Our study highlights the life-threatening nature of TLS, a previously under-recognized oncologic emergency of breast cancer, especially in patients with extensive liver metastases. Emergency room physicians should consider TLS as a differential diagnosis when evaluating acute renal failure and electrolyte derangement in patients with metastatic breast cancer, especially in those with diffused liver metastases.
Bibliography
1. Howard SC., et al. “The tumor lysis syndrome”. The New England Journal of Medicine 364 (2011): 1844-1854.
2. Harmon J., et al. “The Clinical Features, Outcome and Prognosis of Spontaneous Tumor Lysis Syndrome in Solid Tumor”. Journal of Oncology Research Forecast 1.2 (2018): 1009.
3. Cordrey EO and Wang J. “Tumor Lysis Syndrome Associated with Immune Checkpoint Blockade in Solid Tumors”. Japanese Journal of Cancer and Oncology Research 1.1 (2018): 1005.
4. Harmon J., et al. “Liver Metastasis is an Independent Predictor for Mortality in Patients Who Developed Tumor Lysis Syndrome: Analysis of 132 Patients with Solid Tumors”. Journal of Clinical Oncology 36.15 (2018): e18766.
5. Brunnhoelzl D and Wang J. “Acute Tumor Lysis Syndrome after Anti-PD1 Immunotherapy Nivolumab for Metastatic Melanoma”. Journal of Molecular Oncology Research 1.1 (2017): 5-6.
6. Goyal H., et al. “Spontaneous fatal recurrent tumor lysis syndrome in ductal breast carcinoma”. Community Oncology 9.4 (2012): 136-137.
7. Elfar A., et al. “Spontaneous tumor lysis syndrome in breast cancer: a case report and discussion”. Journal of Cancer Therapeutics and Research 2 (2013):
8. Sklarin NT and Markham M. “Spontaneous recurrent tumor lysis syndrome in breast cancer”. American Journal of Clinical Oncology 18.1 (1995): 71-73.
9. American Cancer Society. “Breast Cancer Facts and Figures”. American Cancer Society, Inc Atlanta: 2009-2010.
10. Richards MA., et al. “Influence of delay on survival in patients with breast cancer: a systematic review”. Lancet 353.9159 (1999): 1119-1126.
11. Jassem J., et al. “Delays in diagnosis and treatment of breast cancer: a multinational analysis”. European Journal of Public Health 24.5 (2014): 761-776.
12. Baudon C., et al. “Tumor lysis syndrome following trastuzumab and pertuzumab for metastatic breast cancer: a case report”. Journal of Medical Case Reports 10 (2016): 178.
13. Barton JC. “Tumor lysis syndrome in non hematopoietic neoplasms”. Cancer 64.3 (1989): 738-740.
14. Baudon C., et al. “Tumor lysis syndrome following trastuzumab and pertuzumab for metastatic breast cancer: a case report”. Journal of Medical Case Reports 10.1 (2016).
15. Cech P., et al. “Tumor Lysis Syndrome after Tamoxifen Flare”. The New England Journal of Medicine 315.4 (1986): 263-264.
16. Drakos P., et al. “Tumor lysis syndrome in nonhematologic malignancies. Report of a case and review of the literature”. American Journal of Clinical Oncology 17.6 (1994): 502-505.
17. Kurt M., et al. “Tumor lysis syndrome following a single dose of capecitabine”. Annals of Pharmacotherapy 38.5 (2004): 902-902.
18. Mott FE., et al. “Tumor Lysis Syndrome in Solid Tumors”. Supportive Cancer Therapy 2.3 (2005): 188-191.
19. Rostom AY., et al. “Tumor lysis syndrome following hemi-body irradiation for metastatic breast cancer”. Annals of Oncology 11.10 (2000): 1349-1351.
20. Stark ME., et al. “Fatal acute tumor lysis syndrome with metastatic breast carcinoma”. Cancer 60.4 (1987): 762-764.
21. Taira F., et al. “Tumor lysis syndrome following trastuzumab for breast cancer: a case report and review of the literature”. Breast Cancer 22.6 (2015): 664-668.
22. Üstündağ Y., et al. “Acute tumor lysis syndrome associated with paclitaxel”. Annals of Pharmacotherapy 31.12 (1997): 1548-1549.
23. Vaidya GN and Acevedo R. “Tumor lysis syndrome in metastatic breast cancer after a single dose of paclitaxel”. The American Journal of Emergency Medicine 33.2 (2015): 308.e1-308.e2.
24. Cordrey EO., et al. “Spontaneous Tumor Lysis Syndrome in a Giant Neglected Breast Cancer”. Journal of Molecular Oncology Research 2.2 (2018): 1-4.
25. Kaplan GG., et al. “Acute hepatic failure and multi-system organ failure secondary to replacement of the liver with metastatic melanoma”. BMC Cancer 5.1 (2005).
26. Frestad D., et al. “Acute onset and rapid progression of multiple organ failure in a young adult with undiagnosed disseminated colonic adenocarcinoma”. Case Reports (2014).
Volume 4 Issue 1 January 2020
©All rights reserved by Britney Bell and Jue Wang.